.
“As an undergraduate student in psychology, I was taught that multiple personalities were a very rare and bizarre disorder. That is all that I was taught on ... It soon became apparent that what I had been taught was simply not true. Not only was I meeting people with multiplicity; these individuals entering my life were normal human beings with much to offer. They were simply people who had endured more than their share of pain in this life and were struggling to make sense of it.”
― Deborah Bray Haddock, The Dissociative Identity Disorder Sourcebook
Validity
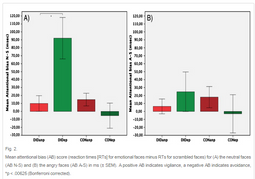
Image Description: Mean attentional bias (AB) score (reaction times [RTs] for emotional faces minus RTs for scrambled faces) for (A) the neutral faces (AB N-S) and (B) the angry faces (AB A-S) in ms (± SEM). A positive AB indicates vigilance, a negative AB indicates avoidance, *p < .00625 (Bonferroni corrected).
Yolanda R. Schlumpf, Ellert R.S. Nijenhuis, Sima Chalavi, Ekaterina V. Weder, Eva Zimmermann, Roger Luechinger, Roberto La Marca, A.A.T. Simone Reinders, Lutz Jäncke, Dissociative part-dependent biopsychosocial reactions to backward masked angry and neutral faces: An fMRI study of dissociative identity disorder, NeuroImage: Clinical, Volume 3, 2013, Pages 54-64, ISSN 2213-1582, http://dx.doi.org/10.1016/j.nicl.2013.07.002.
One major support for DID as a traumagenic disorder is the strong association between DID and childhood trauma. DID patients have smaller hippocampal and amygdalar glands, something seen in those who were abused as children and have posttraumatic stress disorder (PTSD) (Vermetten, Schmahl, Linder, Loewenstein, & Bremme, 2006).1 As well, one study confirmed childhood abuse in eight out of nine cases of DID and all twelve cases of DDNOS (OSDD-1) examined (Coons, 1994).2 At least 79% of those with DID meet the criteria for PTSD (Ellason, Ross, & Fuchs, 1996)3, though other studies place the number at 89% (Brand et al., 2009).4 Another study found that 98.1% of individuals with DID experienced child abuse (Ellason & Ross, 1997).5 Despite these findings, DID cannot be said to be the same as PTSD. Individuals with DID and co-morbid PTSD have larger putamen and pallidum volumes compared to individuals with only PTSD with these volumes being positively correlated with severity of dissociative symptoms. Severity of dissociative symptoms is also negatively correlated with volume of the inferior parietal cortex (Chalavi et al., 2015).6
Another important point is the difference between trauma-oriented and non-trauma-oriented alters. The current theory for the formation of DID, the theory of structural dissociation, relies on the existence of both trauma oriented emotional parts (EP) and daily life oriented apparently normal parts (ANP), and various studies reinforce that these parts are distinct. It's been shown that ANP (also called neutral identity states, or NIS) and EP (also called trauma-related identity states, or TIS) have different neural resting state activity, with EP being more likely to activate brain regions involved in self-referencing and sensorimotor actions (Schlumpf et al., 2014).7 When exposed to trauma scripts, NIS activate areas in the cerebral cortex while TIS activate subcortical areas. NIS brain network activation patterns are similar to those displayed by healthy individuals who are emotionally suppressing unwanted memories. In contrast, TIS brain network activation patterns indicate unsuppressed memory retrieval associated with acute stress. This supports that TIS but not NIS relate traumatic autobiographical memories to themselves (Reinders, Willemsen, Vos, Boer, & Nijenhuis, 2012).8 Similarly, EP compared to ANP are over-reactive towards angry and neutral preconsciously perceived faces and in response demonstrate more activation of the right parahippocampal gyrus, an area of the brain associated with recall of autobiographical memories and with re-experiencing symptoms for individuals with PTSD (Schlumpf et al., 2013).9
In none of these studies are individuals without DID able to match the differences between trauma oriented and non-trauma oriented parts even if the control individuals are highly fantasy prone. In fact, the low fantasy prone individuals studied better imitate the neural reactions of NIS versus TIS to trauma scripts. The same study finds that individuals with DID are not more fantasy prone than the general population, a finding that refutes the idea that DID is caused by fantasy proneness or suggestibility (Reinders, Willemsen, Vos, Boer, & Nijenhuis, 2012).8
1 Vermetten, E., Schmahl, C., Lindner, S., Loewenstein, R., & Bremner, J. (2006). Hippocampal and amygdalar volumes in Dissociative Identity Disorder. American Journal of Psychiatry, 163(4), 630-636. doi: 10.1176/appi.ajp.163.4.630
2 Coons, P. (1994). Confirmation of childhood abuse in child and adolescent cases of multiple personality disorder and dissociative disorder not otherwise specified [Abstract]. The Journal of Nervous and Mental Disease, 182(8), 461-4. doi: 10.1097/00005053-199408000-00007
3 Ellason, J., Ross, C., & Fuchs, D. (1996). Lifetime Axis I and II comorbidity and childhood trauma history in dissociative identity disorder. Psychiatry: Interpersonal and Biological Processes, 59(3), 255-266.
4 Brand, B., Classen, C., Lanins, R., Loewenstein, R., McNary, S., Pain, C., Putnam, F. (2009). A naturalistic study of dissociative identity disorder and dissociative disorder not otherwise specific patients treated by community clinicians. Psychological Trauma: Theory, Research, Practice, and Policy, 1(2), 153-171. doi: 10.1037/a0016210
5 Ellason, J., & Ross, C. (1997). Two-year follow-up of inpatients with Dissociative Identity Disorder. American Journal of Psychiatry, 154(6), 832-839. Retrieved from http://www.rossinst.com/treatment_outcome.html
6 Chalavi, S., Vissia, E. M., Giesen, M. E., Nijenhuis, E. R., Draijer, N., Barker, G. J., . . . Reinders, A. A. (2015). Similar cortical but not subcortical gray matter abnormalities in women with posttraumatic stress disorder with versus without dissociative identity disorder. Psychiatry Research: Neuroimaging, 231(3), 308-319. doi:10.1016/j.pscychresns.2015.01.014
7 Schlumpf, Y. R., Reinders, A. A., Nijenhuis, E. R., Luechinger, R., Osch, M. J., & Jäncke, L. (2014). Dissociative part-dependent resting-state activity in dissociative identity disorder: A controlled fMRI perfusion study. PLoS ONE, 9(6). doi:10.1371/journal.pone.0098795
8 Reinders, A. A., Willemsen, A. T., Vos, H. P., Boer, J. A., & Nijenhuis, E. R. (2012). Fact or factitious? A psychobiological study of authentic and simulated dissociative identity states. PLoS ONE, 7(6). doi:10.1371/journal.pone.0039279
9 Schlumpf, Y. R., Nijenhuis, E. R., Chalavi, S., Weder, E. V., Zimmermann, E., Luechinger, R., . . . Jäncke, L. (2013). Dissociative part-dependent biopsychosocial reactions to backward masked angry and neutral faces: An fMRI study of dissociative identity disorder. NeuroImage: Clinical, 3, 54-64. doi:10.1016/j.nicl.2013.07.002
This website uses cookies in order to analyze visitor trends. Identifying or personal information is not collected on this website, and the data collected is not sold to or shared with third party services. For more information on the data that this website collects and how to opt out, please visit the Privacy Policy page. Continued use of the website indicates agreement with this policy.
All content on this website is provided for the purpose of general information only. It is not intended to be used as a substitute for professional diagnosis and treatment. Please consult a licensed professional before making any healthcare decisions or for guidance about potential mental health conditions.
This website was last updated 6/22/2024.
This page was last updated 3/9/2017.
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License by Katherine Reuben.